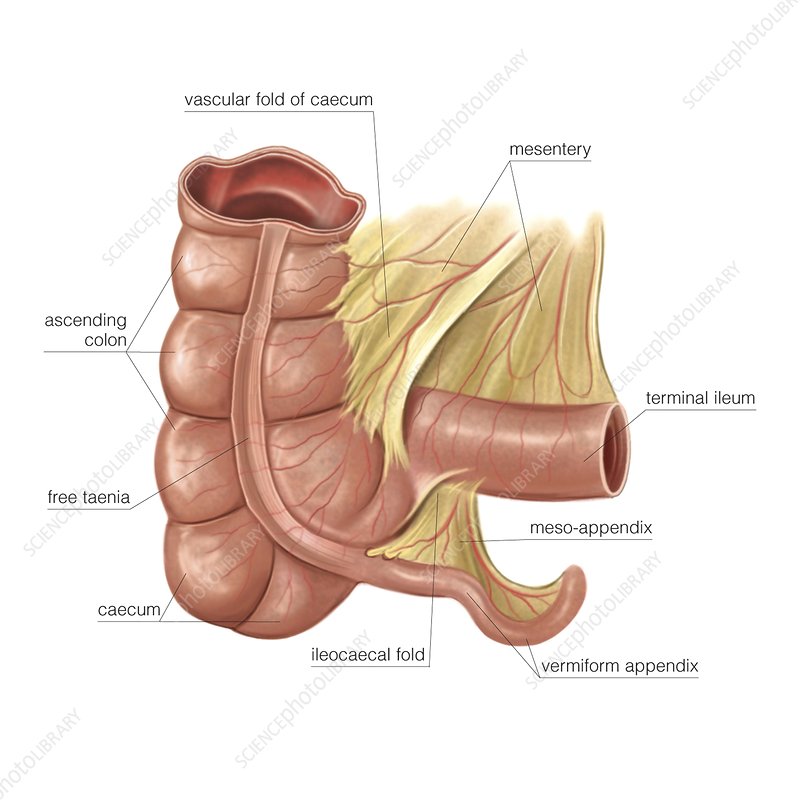
Anatomically, the appendix is a closed-ended, narrow, worm-like tube up to several inches in length that attaches to the cecum (the first part of the colon). The inner lining of the appendix produces a small amount of mucus that flows through the open central core of the appendix and into the cecum. The wall of the appendix contains lymphatic tissue that is part of the immune system.
It is not clear if the appendix has an important role in the body in older children and adults. In young children it may have an immune function. There are no major, long-term health problems resulting from removing the appendix although a slight increase in some diseases has been noted, for example, Crohn’s disease.
Despite diagnostic and therapeutic advancement in medicine, appendicitis remains a clinical emergency and is one of the common causes of acute abdominal pain
WHAT IS APPENDICITIS?
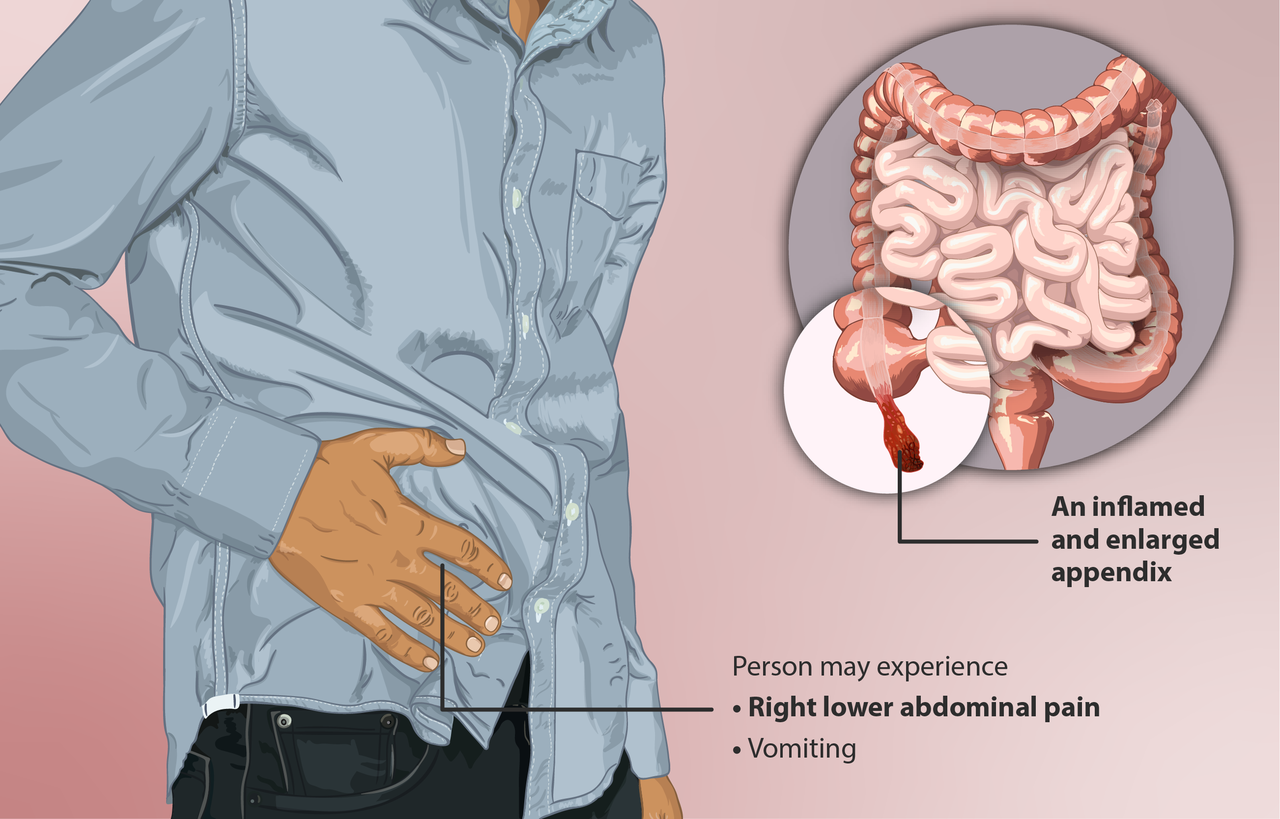
Appendicitis means inflammation of the appendix, which becomes infected with bacteria from the intestine and gradually swells and fill with pus. If untreated, the swollen appendix might burst with pus contamination of the abdominal cavity. This can cause a serious infection of the membrane that lines the abdomen (peritonitis), or an abscess in the abdomen. So, if appendicitis is suspected, early treatment is essential before it bursts.
WHAT ARE THE SYMPTOMS OF APPENDICITIS?
• Pain in the abdomen (tummy pain)
• commonly starts in the middle of the abdomen, non-specific discomfort or pain
• Over the next few hours the pain typically ‘travels’ to the lower right hand side of the
• Gradually the severity of pain increases over 6-24 hours.
• The pain tends to be more sharp if you cough or make any movements.
• The pain may ease a bit if you pull your knees up towards your chest.
• The lower abdomen is usually tender, particularly in the lower right hand side.
• If the appendix perforates (bursts) then severe pain can spread to all the abdomen
Other symptoms that may occur include the following.
• Anorexia (loss of appetite) that may worsen over time and can result in nausea and vomiting.
• Fever and generally feeling unwell.
• Constipation may occur. Sometimes diarrhoea
• Frequent passing of urine may develop (due to the inflammation ‘irritating’ the nearby ureter (the tube between the kidney and bladder).
However, the clinical presentation of appendicitis is notoriously inconsistent as the classic history of anorexia and periumbilical pain followed by nausea, right lower abdomen pain, and vomiting occurs in only 50% of cases. Therefore, it is important have high clinical suspicion with the aids of blood test and imaging test to reach the diagnosis for early treatment to prevent complication.
Who are more at risk of getting appendicitis?
• The incidence of appendicitis gradually rises from birth, peaks in the late teen years, and gradually declines in the geriatric years. The mean age when appendicitis occurs in the pediatric population is 6-10 years. Younger children have a higher rate of perforation, with reported rates of 50-85%. Although rare, neonatal and even prenatal appendicitis have been reported. Clinicians must maintain a high index of suspicion in all age groups.
How true is the old wives tale about doing sports as a cause of appendicitis?
It is not true as the cause of acute appendicitis is usually due to blockage of its lumen. The most common causes of luminal obstruction include lymphoid hyperplasia secondary to inflammatory bowel disease (IBD) or infections (more common during childhood and in young adults), fecal stasis and fecaliths (more common in elderly patients), parasites (especially in Eastern countries), or, more rarely, foreign bodies and neoplasms.
How does someone get a diagnosis? – Common scans and diagnosis procedures.
The diagnosis of appendicitis begins with a thorough history and physical examination. Patients often have fever and there usually will be moderate to severe tenderness in the right lower abdomen when the doctor pushes there. If inflammation has spread to the peritoneum, there is frequently rebound tenderness. Rebound tenderness is pain that is worse when the doctor quickly releases his or her hand after gently pressing on the abdomen over the area of tenderness.
Common test:
1) White blood cell count
– The white blood cell count usually becomes elevated with infection.
2) Urinalysis
– Urinalysis is a microscopic examination of the urine that detects red blood cells, white blood cells and bacteria in the urine. Urinalysis usually is abnormal when there is inflammation or stones in the kidneys or bladder. The urinalysis also may be abnormal with appendicitis because the appendix lies near the ureter and bladder. If the inflammation of appendicitis is great enough, it can spread to the ureter and bladder leading to an abnormal urinalysis. Most patients with appendicitis, however, have a normal urinalysis. Therefore, a normal urinalysis suggests appendicitis more than a urinary tract problem.
3) Urine pregnancy test
-For women of childbearing age, the level of urinary beta–human chorionic gonadotropin (beta-hCG) is useful in differentiating appendicitis from early ectopic pregnancy.
Imaging studies
1) Ultrasound
– An ultrasound is a painless procedure that uses sound waves to provide images to identify organs within the body. Ultrasound can identify an enlarged appendix or an abscess. Nevertheless, during appendicitis, an enlarged inflamed appendix or abscess can be seen in only 50% of patients. Therefore, not seeing the appendix during an ultrasound does not exclude appendicitis. Ultrasound also is helpful in women because it can exclude the presence of conditions involving the ovaries, Fallopian tubes and uterus (pelvic inflammatory disease, PID) that can mimic appendicitis.
2) Computerized tomography (CT) scan
In patients who are not pregnant, a CT scan of the area of the appendix is useful in diagnosing appendicitis and peri-appendiceal abscesses as well as in excluding other diseases inside the abdomen and pelvis that can mimic appendicitis.
Concerns have grown over the possible adverse effects on patients from exposure to radiation from CT scanning. Ultrasonography may offer a safer alternative as a primary diagnostic tool for appendicitis, with CT scanning used in those cases in which ultrasonograms are negative or inconclusive.
Diagnostic laparoscopy as last resort if origin of abdominal pain still uncertain
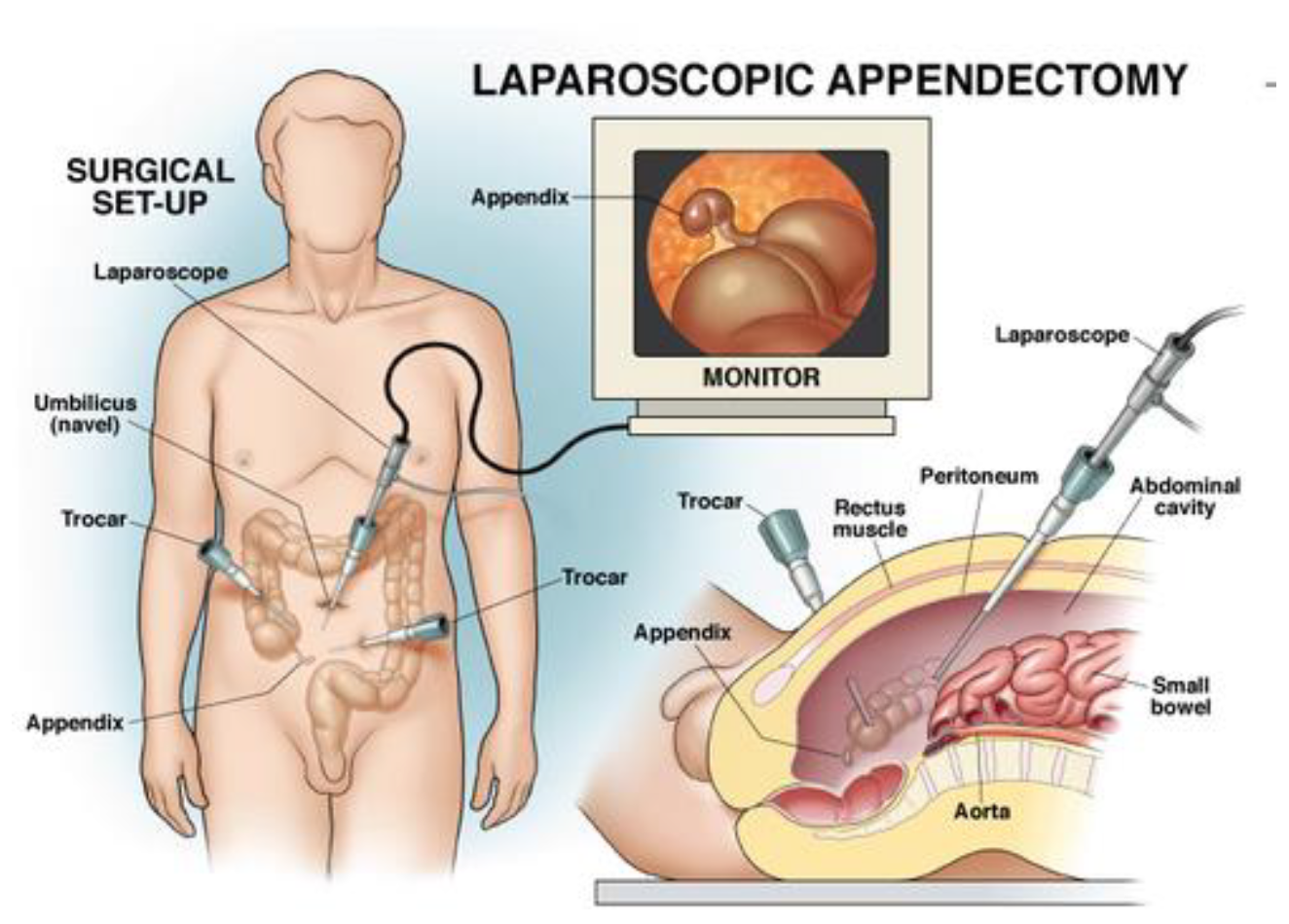
- Laparoscopy is a surgical procedure in which a small fiberoptic tube with a camera is inserted into the abdomen through a small puncture made on the abdominal wall. Laparoscopy allows a direct view of the appendix as well as other abdominal and pelvic organs. If appendicitis is found, the inflamed appendix can be removed with the laparoscope. The disadvantage of laparoscopy compared to ultrasound and CT is that it requires a general anesthetic.
There is no one test that will diagnose appendicitis with certainty. Therefore, the approach to suspected appendicitis may include a period of observation, tests as previously discussed, or surgery.
What are the health threats/complications of an untreated appendicitis or a rupture?
Appendicitis means inflammation of the appendix, which becomes infected with bacteria from the intestine and gradually swells and fill with pus. If untreated, the swollen appendix might burst with pus contamination of the abdominal cavity. This can cause a serious infection of the membrane that lines the abdomen (peritonitis), or an abscess in the abdomen. Patient can died of severe infection complicated acute appendicitis. Therefore, if appendicitis is suspected, early treatment is essential before it bursts.
Should someone consider doing a appendectomy as a preventive measure?
No. Surgeon will only remove the appendix if it is inflamed and cause abdominal pain. The surgery is call appendicectomy.
2 types of surgery for appendicectomy
2 surgical techniques available:
- Laparoscopic appendicectomy. It is a new minimally invasive surgery with 3 small puncture wounds are needed in the abdomen with small scars remaining afterwards. The operation is performed with the aid of a special telescope that is pushed into the abdomen through small wound. It causes less pain, faster recovery with shorter hospital stays and better cosmetic results
- Open appedicectomy. It isa traditional open surgery to remove the appendix with a larger cut required to remove the appendix, thus much more pain and longer hospital stays. Its indicated for complicated appendicitis with multiple abscess collection at the abdominal cavity.
Laparoscopic surgery offer minimal pain and faster recovery
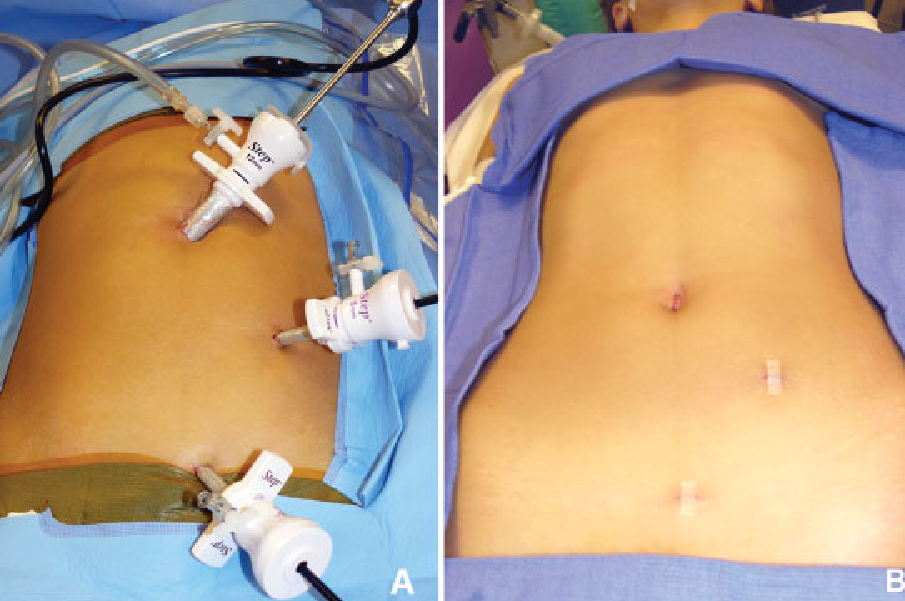
3 small scar left after surgery




